Part 1 – Purpose and Executive Summary
This page reconstructs, in six parts, the court‑ordered Evidence Preservation (証拠保全) session conducted on 8 February 2011 at Toride Kyodo Hospital (now JA Toride Medical Center), under the supervision of the Mito District Court, Ryugasaki Branch. The reconstruction is based on primary materials: a full audio recording, the official Verification Protocol (検証調書), email correspondence with counsel, and contemporaneous notes by the patient’s family.
In principle, evidence preservation is designed to secure critical records and safeguard their evidentiary value before litigation. In this case, however, several features of the session had the effect of narrowing the scope of preserved materials or weakening their formal status:
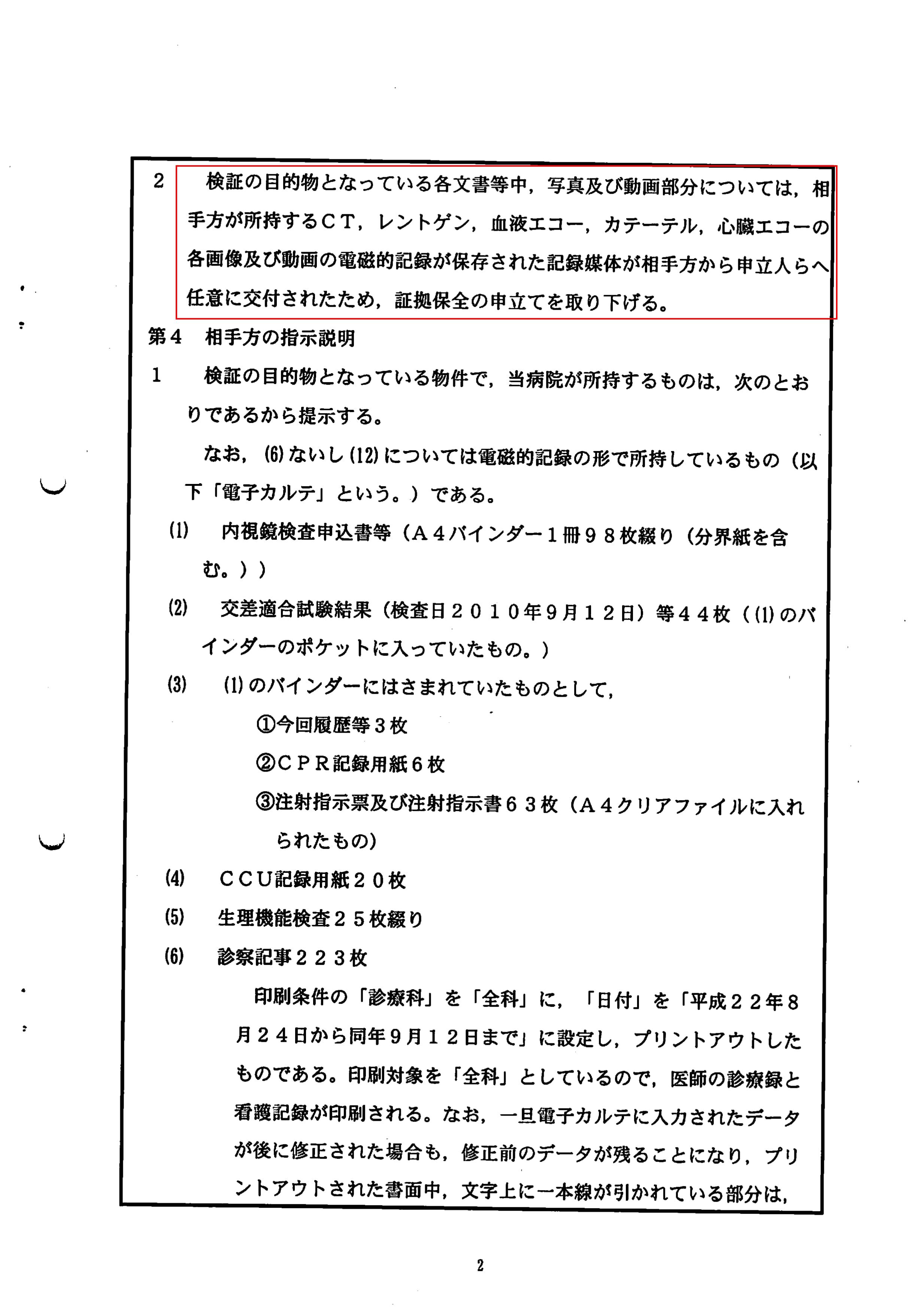
- Key imaging data (PCI and CT) were reclassified as “voluntary disclosures” and removed from the formal preservation motion.
- The list of items to be preserved (the “inventory”) was effectively frozen before all requested records were included.
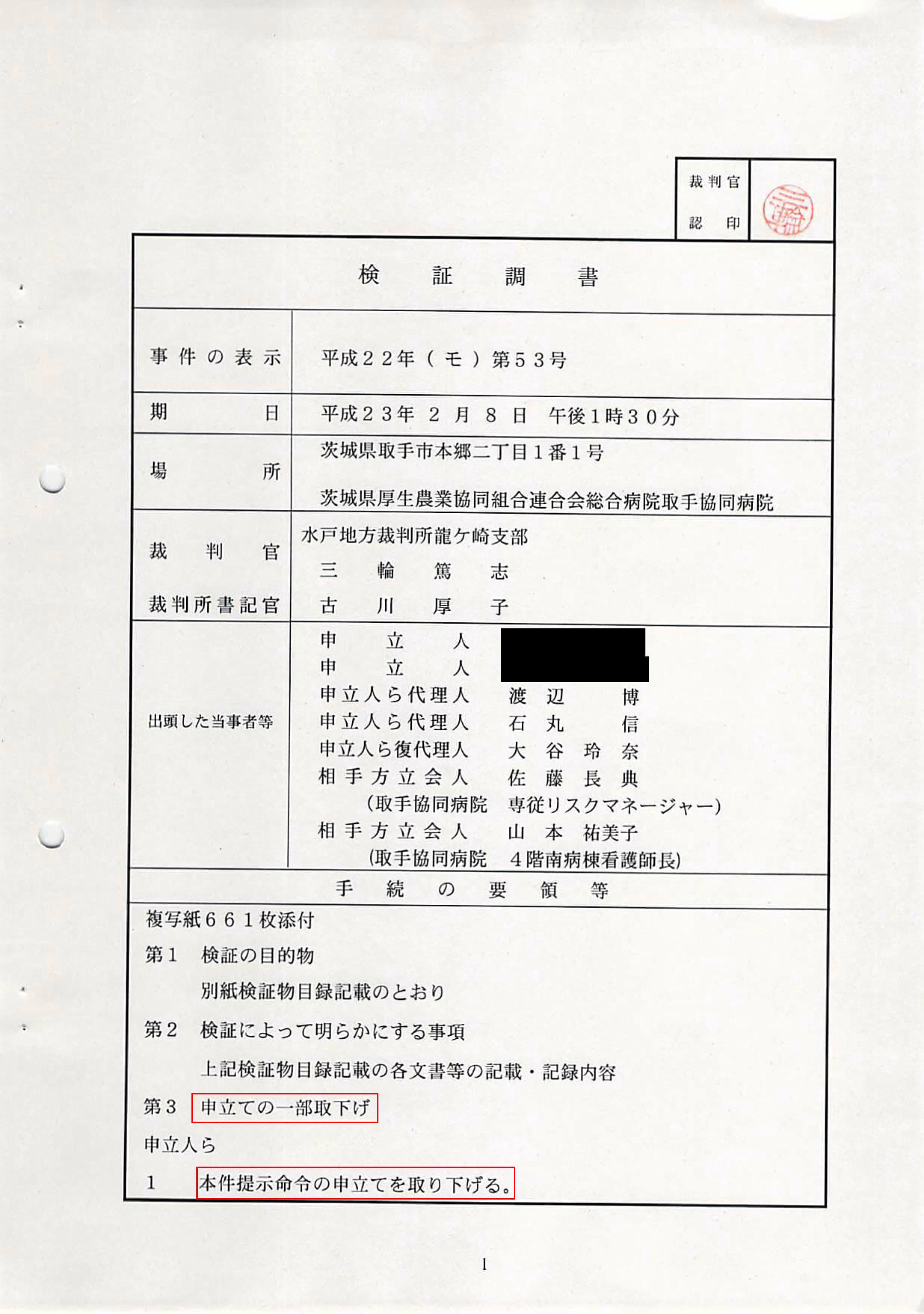
- The official protocol mis‑recorded the identity of attendees and omitted at least one person who was present.
- An alternate‑name ventilator sheet, closely mirroring the patient’s course, was treated as a record to be discarded.
- Requests to obtain ECG, echocardiography data, and ward logs were blocked by counsel during the session.
Part 2 – Legal and Procedural Context
Under Japan’s Code of Civil Procedure, evidence preservation allows a court to secure evidence when there is a risk that it may be lost or altered before a lawsuit is filed. In medical cases, this typically includes:
- On‑site inspection of medical charts, nursing records, and monitoring logs.
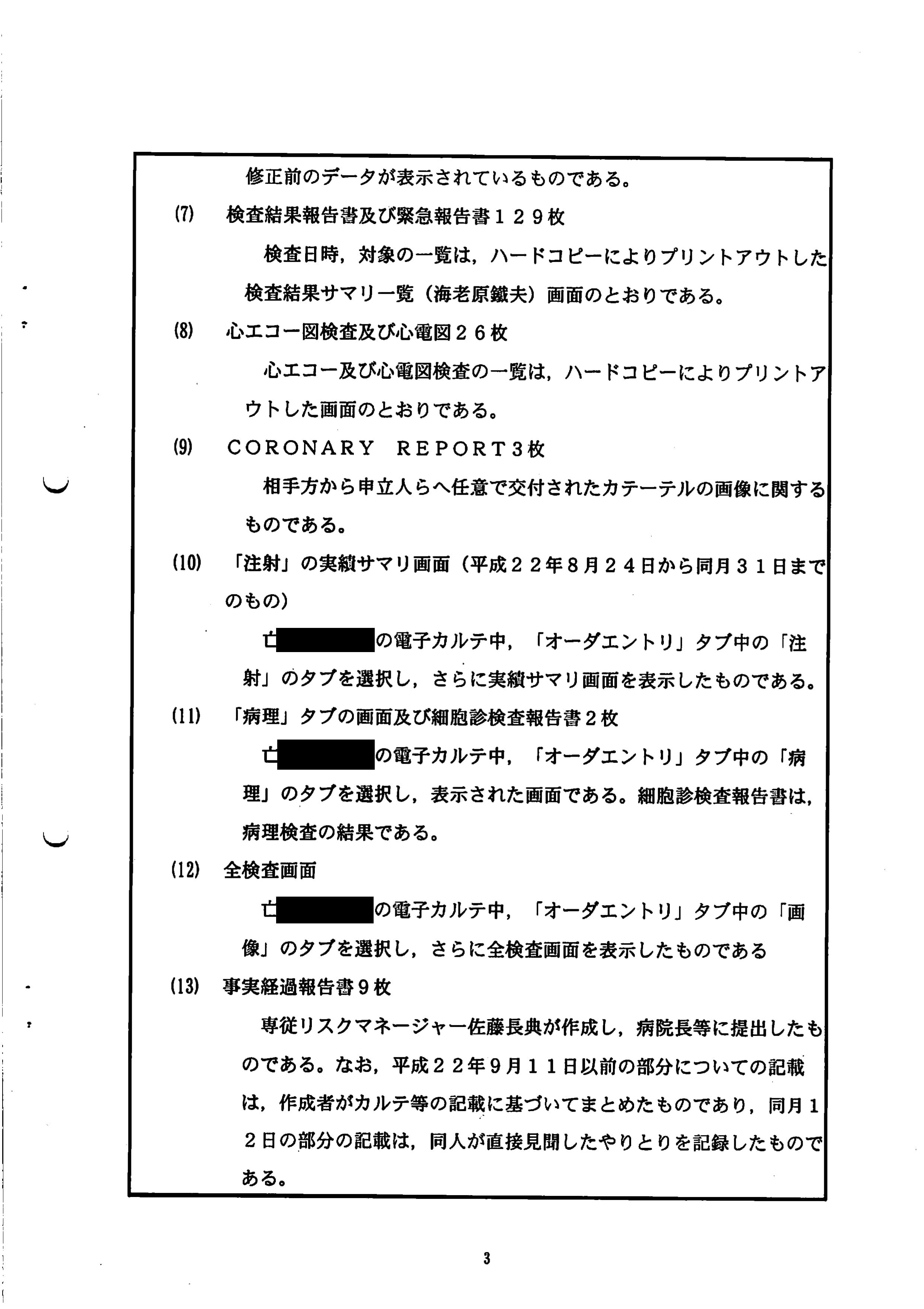
- Copying of imaging data (e.g., PCI, CT, X‑ray, echocardiography) and laboratory results.
- Creation of an official protocol documenting what was inspected, copied, or withdrawn.
In theory, materials obtained through evidence preservation enjoy a clear evidentiary status in later proceedings. Materials treated as “voluntary disclosures” or omitted from the protocol may not benefit from the same level of formal protection. Understanding how this distinction was applied on 8 February 2011 is central to the analysis that follows.
Part 3 – Timeline of the Evidence Preservation Session
The following timeline is reconstructed from the audio recording, the Verification Protocol, and contemporaneous notes. Times are approximate but reflect the sequence of events on 8 February 2011 at Toride Kyodo Hospital.
- The patient’s widow and younger son arrive at the hospital. The elder son does not attend.
- Presiding Judge Atsushi Miwa, a court clerk, hospital representatives, and counsel for the family assemble in a meeting room.
- PCI and CT imaging data are handed over on CD‑R in the room, in the presence of the judge and counsel.
- The judge states that, because the imaging data have been “voluntarily provided,” the corresponding part of the preservation motion can be withdrawn.
- Counsel for the family raise no objection. The family, unfamiliar with the legal implications, do not contest the withdrawal.
- Review of charts and nursing records begins.
- The younger son requests that the 26 August ECG and 27 August echocardiography data be included. Counsel intervenes and stops the request.
- The ward head nurse offers the ward log. Counsel states that it is “not necessary,” and it is not taken into the preserved set.
- A ventilator setting sheet under the alternate name “Tamaki Ishikawa” is identified among the records. Its content closely resembles the patient’s course.
- According to later email correspondence, the court instructs that this alternate‑name sheet be treated as another patient’s record and destroyed.
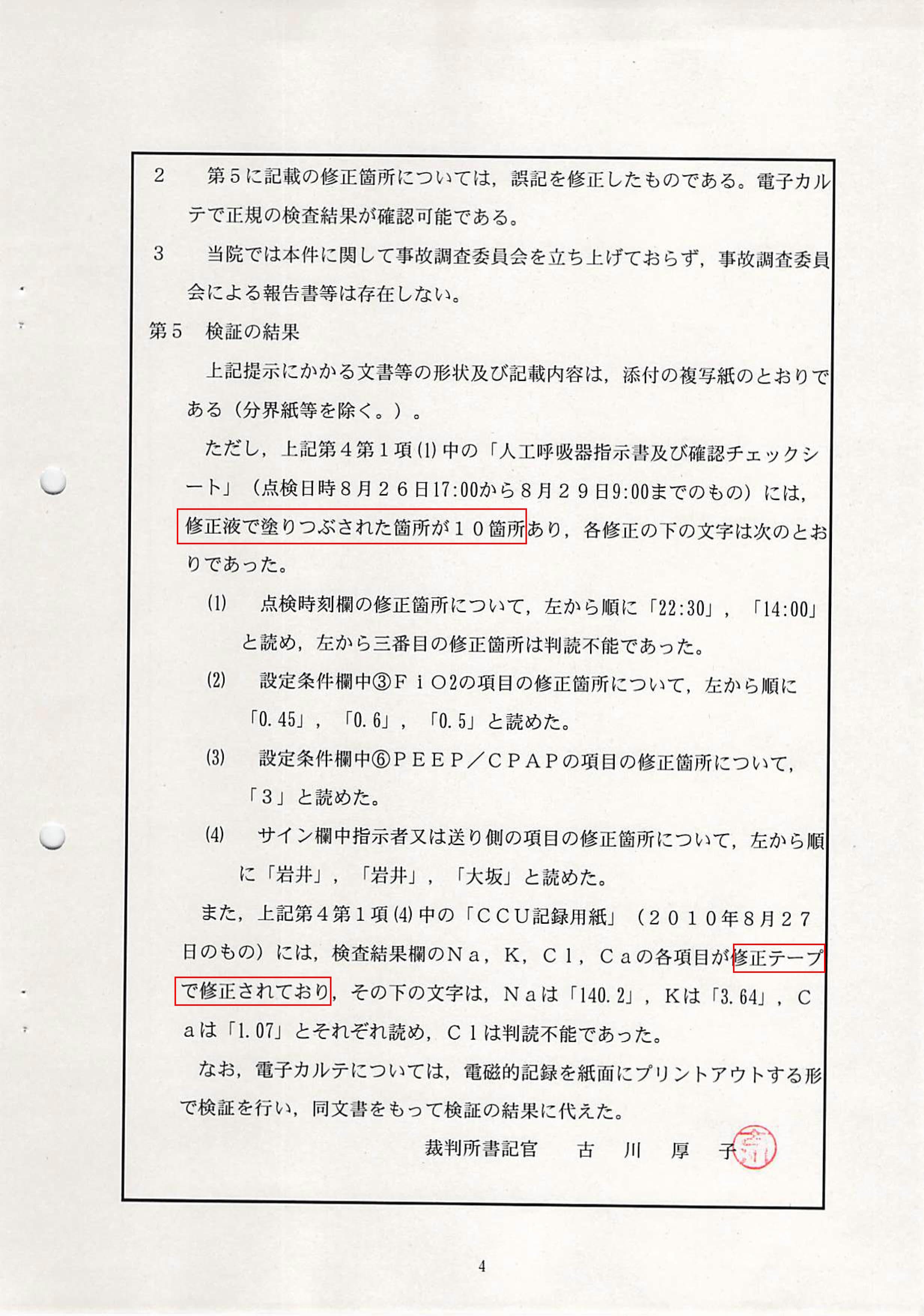
- Multiple uses of correction fluid and correction tape in ICU records and laboratory sheets are noted.
- The on‑site session concludes. The Verification Protocol is later prepared and issued by the court.
This timeline provides the factual backbone for the evidence‑based analysis in Part 4 and the structural review in Part 5.
Part 4 – Evidence‑Based Analysis (Explanations vs. Primary Records)
This section compares explanations given during or around the session with what is documented in primary records (audio, protocol, and correspondence), using a “narrative vs. evidence” structure common in investigative reporting.
4.1 Inventory of Requested Items vs. Actual Preservation Scope
- Counsel’s explanation: The family was told that evidence preservation would “comprehensively” secure the medical records, and that the precise wording of the inventory was not critical.
- Primary records: Items not explicitly listed—such as the 26 August ECG, the 27 August echocardiography data, and the ward log—were not preserved. The audio shows that attempts to add them were blocked, and the protocol reflects only the narrower set.
4.2 Reclassification of Imaging Data as “Voluntary Disclosures”
- On‑record statement: The judge notes that PCI and CT data have been “voluntarily provided” and proposes that the corresponding part of the motion be withdrawn.
- Primary records: The Verification Protocol’s section on “Partial Withdrawal of Motion” records that imaging data were treated as voluntary disclosures rather than as court‑secured evidence. This removes them from the formal preservation framework, despite their central importance to the case.
4.3 Mis‑recorded Attendance in the Verification Protocol
- Protocol entry: The “Present Parties” section lists the elder son, who did not attend, and omits the younger son, who did.
- Primary records: The audio and family notes confirm that the widow and younger son were present. The mis‑recording affects a basic element of the official document: who actually attended the court‑supervised session.
4.4 Alternate‑Name Ventilator Sheet (“Tamaki Ishikawa”)
- Fact pattern: A ventilator setting sheet under the name “Tamaki Ishikawa” is found among the patient’s records. Its parameters and time course closely mirror those of the patient, with only limited differences.
- Counsel’s email: Counsel later informs the family that the court has requested the sheet be shredded as “another patient’s record.”
- Family’s position: The family asks that the court be informed of the possibility that this sheet represents a pre‑correction version of the patient’s record and that it be preserved.
- Outcome: Counsel replies that the evidentiary value would not change whether the court holds the sheet or not, and no further action is taken to preserve it within the court archive.
4.5 Blocking of Additional Record Requests
- ECG and echocardiography: When the younger son requests inclusion of the 26 August ECG and 27 August echocardiography, counsel intervenes and stops the request.
- Ward log: When the ward head nurse offers the ward log, counsel states that it is “not necessary,” and it is not added to the preserved set.
- Implication: These records are central to reconstructing the clinical course, yet they are excluded not by court refusal but by counsel’s filtering.
4.6 Unlisted Attendee
- Observation: An additional male attendee, wearing a brown suit, is present throughout the session but does not speak on the audio recording.
- Protocol: The Verification Protocol does not list this person in the “Present Parties” section, leaving his identity and role undocumented.
Part 5 – Structural Issues Identified
Taken together, the patterns described above suggest structural issues that go beyond isolated errors or misunderstandings. Key themes include:
-
1. Divergence between the purpose of evidence preservation and its implementation
The session narrowed, rather than maximized, the scope of preserved evidence: imaging data were reclassified as voluntary, additional records were blocked, and the inventory was not expanded despite specific requests. -
2. Filtering of requests by counsel
The family’s attempts to secure ECG, echocardiography, and ward logs were stopped by their own legal representatives, not by the court or the hospital, raising questions about how client instructions were translated into procedural action. -
3. Ambiguity in the status of critical digital evidence
PCI and CT data—central to any analysis of the case—were treated as “voluntary disclosures,” weakening their formal status within the court’s evidentiary framework. -
4. Reliability of official documentation
Mis‑recorded attendance, unlisted participants, and the handling of the alternate‑name ventilator sheet all affect the perceived reliability of the Verification Protocol as a complete and accurate record. -
5. Transparency and traceability
The combination of unlisted attendees, undocumented filtering of requests, and the destruction of a potentially relevant record complicates later efforts to reconstruct what happened and why.
These issues are presented here as structural observations, grounded in primary materials, for consideration by legal scholars, medical safety experts, and investigative journalists.
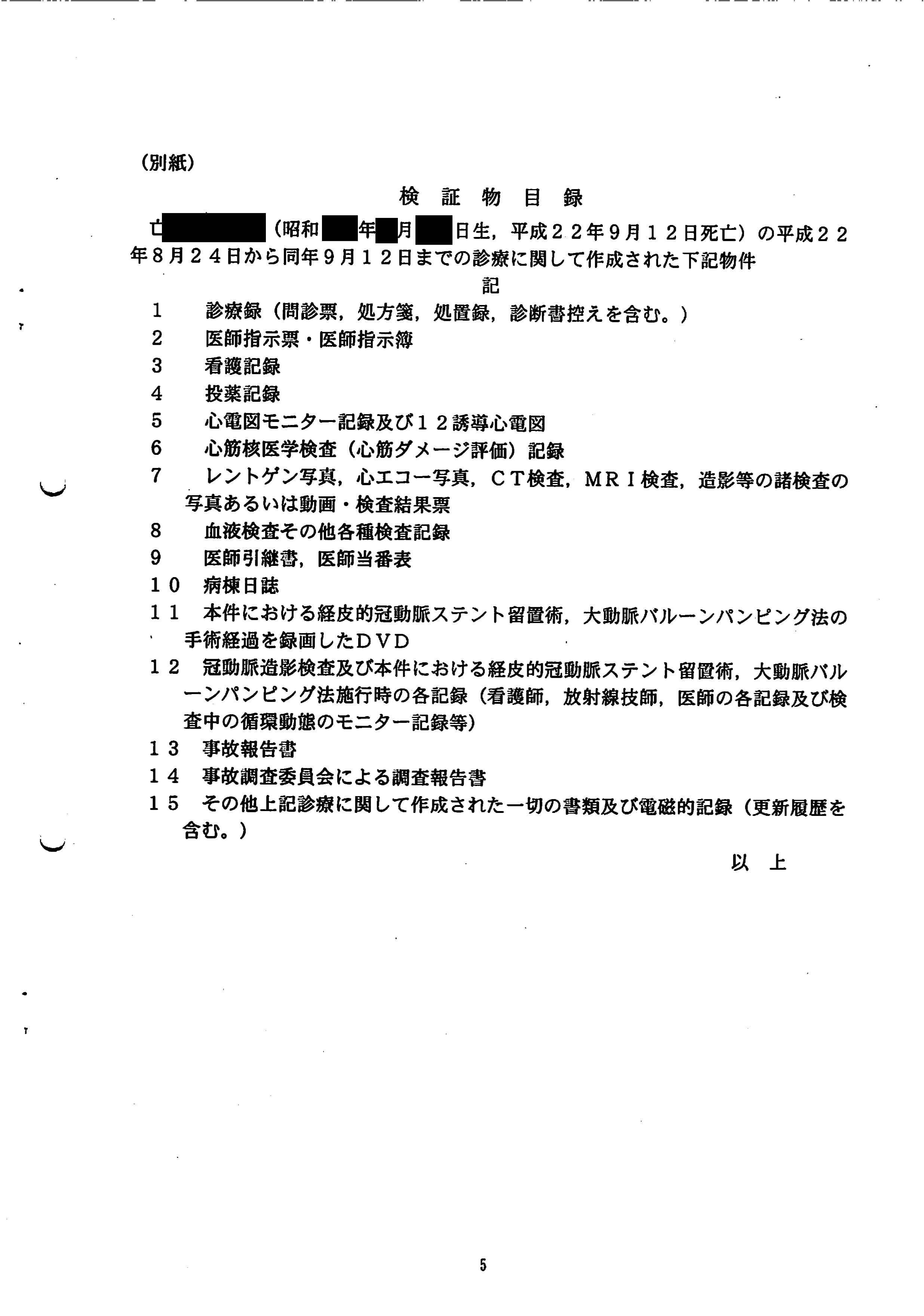
Part 6 – Primary Materials and Document Scans
The reconstruction on this page is based on the following primary materials, preserved with cryptographic hashes to detect any alteration:
- Full audio recording of the 8 February 2011 evidence preservation session.
- Five‑page Verification Protocol (検証調書) issued by the Mito District Court, Ryugasaki Branch.
- Email correspondence with counsel regarding the inventory, imaging data, and the alternate‑name ventilator sheet.
- Contemporaneous notes and timeline prepared by the patient’s widow and younger son.
- Ventilator setting records, including the sheet under the alternate name “Tamaki Ishikawa.”
- ICU and CCU records showing the use of correction fluid and correction tape on key laboratory values.
- Internal notes on the handover and classification of PCI and CT imaging data.
Selected scans of the Verification Protocol are reproduced below to allow independent examination of layout, seals, and formatting:
Additional materials can be made available in a structured format for judicial, academic, or investigative review upon request.